The practices that pull ahead aren’t billing more than anyone else. They’re collecting faster, cleaner and with far less manual effort. Here’s how, and why it matters more now than ever.
Samantha Wagner is EVP and Chief Administrative Officer at Advantum Health.
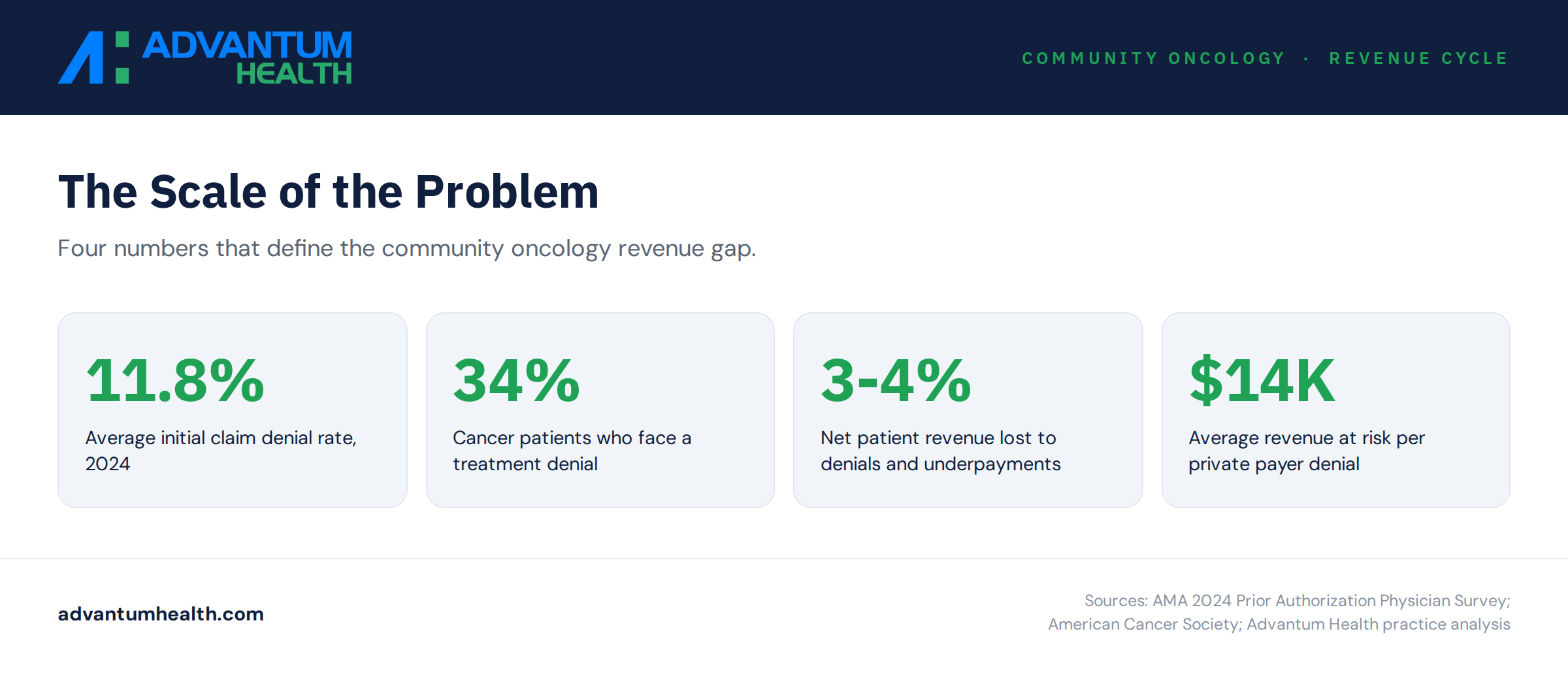
Let me start with the conclusion. Community oncology practices do not have a revenue problem. They have a speed and accuracy problem. The money is already earned. It sits in claims that move too slowly, get keyed by hand, bounce back as denials and quietly get underpaid. What separates the practices that thrive is working harder on their billing. It is intelligent automation doing the repetitive work flawlessly, so revenue arrives faster and people are freed to make the decisions only people can make. That shift is the whole game, and I want to walk you through it.
What I See in Practice After Practice
When I sit down with a practice administrator, the story is almost always the same. Talented people are spending their days on work that software should be doing. Checking eligibility by hand. Re-keying prior authorizations into payer portals. Calling to check claim status. Posting payments line by line. None of it is clinical. All of it is slow. And every hour spent on manual tasks is an hour not spent on the denials and appeals where real money is recovered.
The cost is bigger than it looks. The administrative drag alone is staggering. The American Medical Association’s 2024 Prior Authorization Physician Survey found that physicians average 39 prior authorization requests a week and lose 13 hours of staff and physician time to them. In oncology, where a single drug claim can carry a five- or six-figure value, that slowness is not just frustrating. It is expensive.
Why Getting Paid Faster Is the Real Story
Speed is margin. Every day a clean claim sits unsubmitted, every week a denial goes unworked, every underpayment that ages past the appeal window, is cash you earned and did not collect.
The math is simple. A practice running 55 to 70 days in accounts receivable is financing its own payers, interest free. A practice that runs under 35 days has the same revenue working for it twice as fast. Same care delivered. Same codes billed. A radically different cash position. When I talk about getting money faster, this is what I mean. Not chasing volume, but collapsing the time between care delivered and dollars in the bank.
Intelligent Automation, Not Just “AI”
Let me clear up a distinction the industry blurs constantly. RPA is not AI, and that difference is the whole point.
Robotic process automation, or RPA, handles the high-volume, rules-based work that eats your team’s day: checking eligibility, submitting prior authorizations, checking claim status, posting payments. It follows rules. It is fast and it never tires, but it is not intelligent. Plenty of vendors put an “AI” label on exactly this kind of automation. It isn’t AI. It is a very good robot.
Real AI does something different. It helps your people make better decisions, faster. By reading patterns across thousands of claims and payer behaviors, it can tell your team which claims are likely to deny and why, which denials are worth working first, where an underpayment is hiding and what the next best step is. The expert still makes the call. But instead of spending an hour digging to figure out what to do, they are handed the answer in seconds. That is what reduces time spent, and it is where the real leverage lives.
So we use both, deliberately. RPA clears the busywork. AI sharpens the judgment. Our people own the decisions that need a human. The right technology in the wrong hands still produces the wrong results: automation without intelligence just makes mistakes faster, and intelligence without expertise is a recommendation no one acts on. Put all three together and you get cleaner claims, faster cash and a team spending its time where it counts.
What Makes Advantum Different
Plenty of vendors will sell you software. Fewer will own the outcome. What sets us apart comes down to three things.
We are built around prevention, not cleanup.
Most revenue is lost upstream, in eligibility, authorization and documentation, so that is where we concentrate our automation and our attention. Catching a problem before it becomes a denial is worth far more than appealing it after the fact.
We specialize in oncology.
Oncology billing is its own discipline, with infusion coding, add-on codes, modifier rules and high-dollar drug claims that punish generic approaches. Our automation and our coders are tuned to it.
We close the loop.
Every denial we work teaches the system. Back-end denial patterns feed back into front-end edits and documentation prompts, so the same mistake does not happen twice. That compounding is where the real efficiency lives.
The result is what every practice leader actually wants. Cleaner claims. Faster cash. Fewer write-offs. And a team freed up to do the work that genuinely needs a human.
A Quick Self-Audit
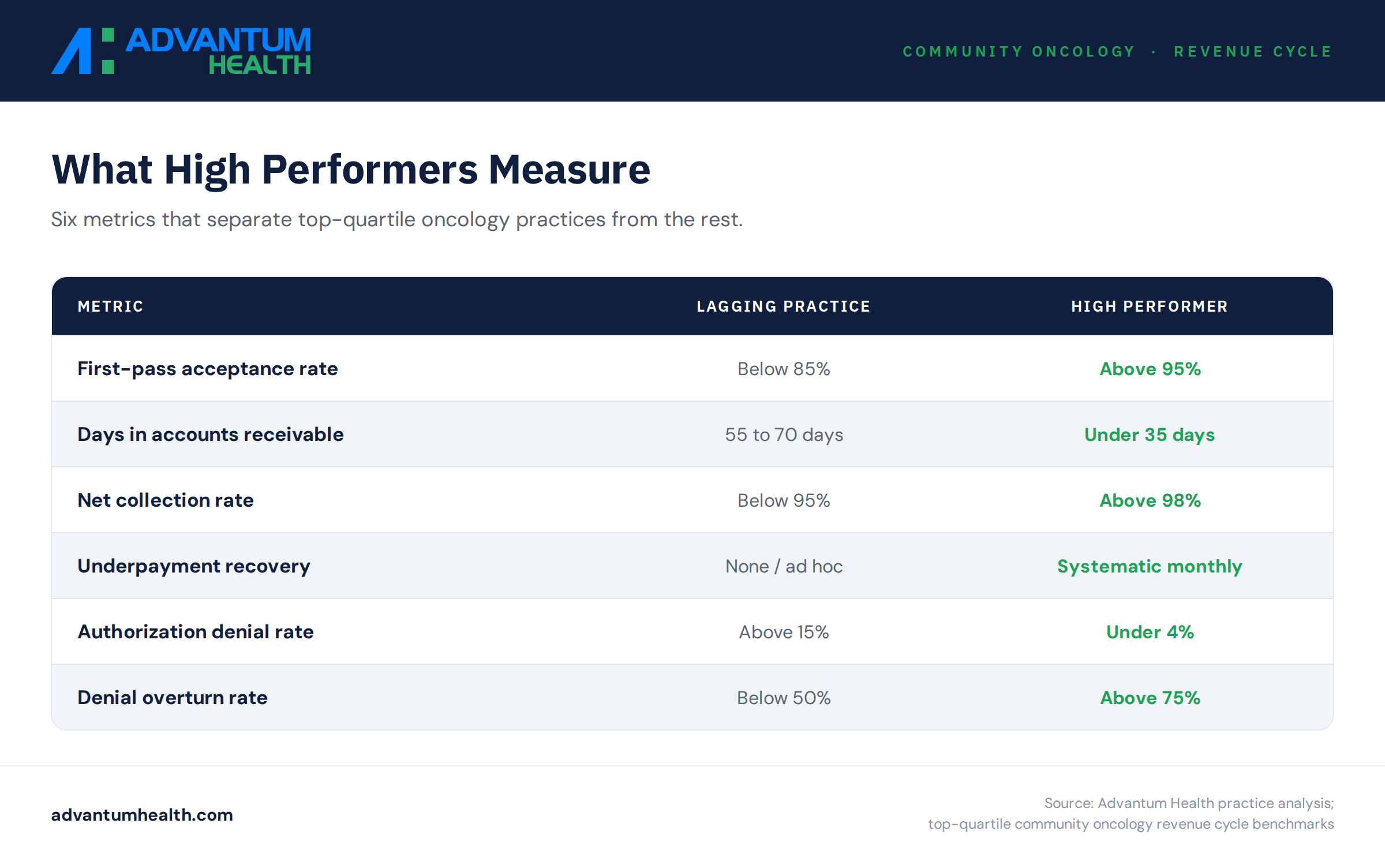
If you want to know where you stand, measure against high performers on six numbers. These are the metrics that separate top-quartile oncology practices from the rest:
First-pass acceptance rate: high performers clear 95 percent; laggards sit below 85 percent.
Days in accounts receivable: high performers stay under 35; laggards run 55 to 70.
Net collection rate: high performers exceed 98 percent; below 95 percent signals leakage.
Underpayment recovery: systematic and monthly for high performers; ad hoc or nonexistent for laggards.
Authorization denial rate: under 4 percent for high performers; above 15 percent is a warning.
Denial overturn rate: high performers overturn more than 75 percent; below 50 percent leaves winnable money on the table.
That last number matters more than most practices realize. A denial is rarely final. In radiation oncology, research published in JAMA Network Open found that the majority of insurance denials are overturned on appeal. If you land on the lagging side of three or more of these, the gap is not theoretical. It is quantifiable, and most of it is recoverable.
Where I Would Start
The practices that win the next decade will be the ones that collect what they have already earned, faster and with less friction. The technology to do that exists today.
If any of this sounds like your practice, I would start where we always start: with a revenue diagnostic. It is a focused lookback at your denials, underpayments and infusion code gaps across your highest-volume payers, and it shows you exactly where the recoverable revenue sits and how much faster you could be collecting it.
Learn more about our prior authorization and eligibility verification services, or read how we approach denial management. When you are ready, let’s talk.